I had a dream this week that I wasn’t wearing a mask. Does that mean I can stop wearing a mask?
Let’s review the current Covid-19 situation. A good source of current information is Dr. Tom Frieden. He’s posted Twitter threads through most of the pandemic as a way of compensating for the muzzled CDC. Even after President Biden unleashed the CDC, Frieden’s threads are still a useful public health summary of the past week.
The winter wave is over, but looks like another wave might be on the way. So, until we understand Covid-19 transmission in a post-vaccine world, yes, I need to wear a mask. For what it’s worth, it seems like we still don’t completely understand Covid-19 transmission in a pre-vaccine world, either.
One reason it seems like we don’t understand Covid-19 transmission is that our understanding of Covid-19 transmission keeps changing. I remember last March watching Youtube videos demonstrating meticulously how to decontaminate groceries. I myself never went full grocery decontamination. I got as far as leaving the groceries outside on the rear porch to air for a day or two, assuming any Covid-19 virus on packages or produce would be inactive by then. I washed my hands more frequently then, and still do, but now I don’t worry about touching my face before I wash my hands.
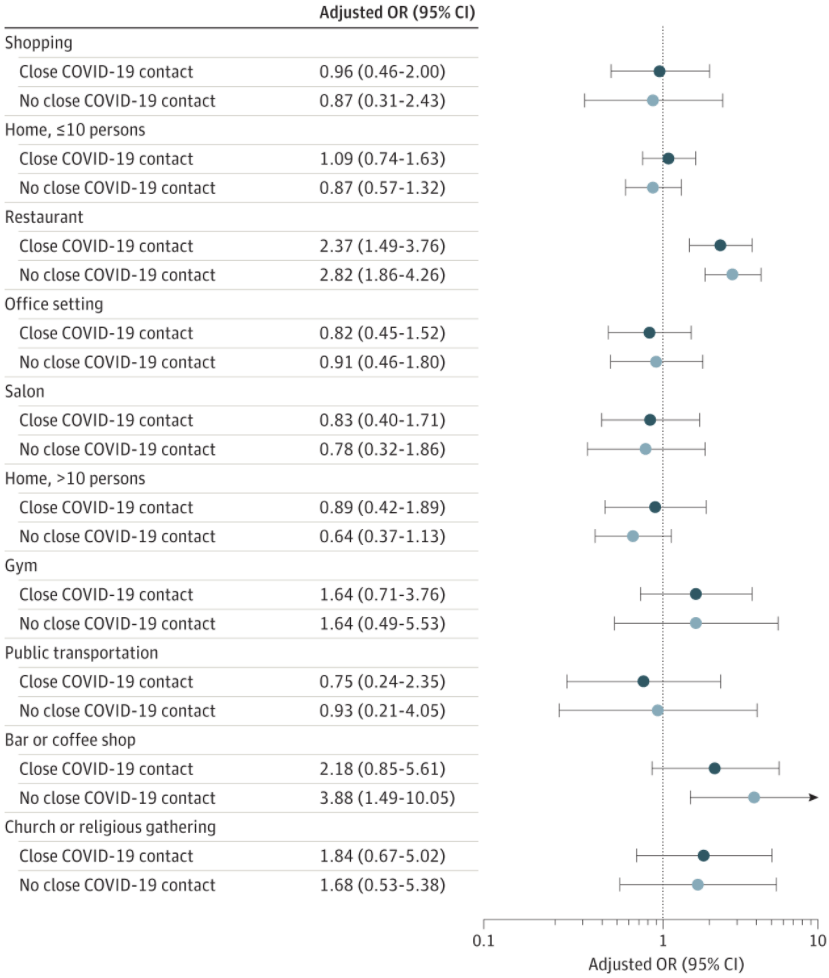
What we do know now that we didn’t know last March is that most Covid-19 transmission is airborne and that superspreader events are the main source of infections. 80% of infections come from 20% of cases. Stop the superspreader events and new cases would drop 80%.
We also understand where superspreader events are likely to occur, namely inside when people don’t wear masks. This chart shows where they are more likely.
Even though we know all this, we still can’t predict superspreader events. Predicting a Covid-19 superspreader event is as hard as predicting when a Boeing 777 will lose an engine. We know a lot of things that might cause an engine to fall off, but that doesn’t mean we can predict when it will happen. In that sense, masks are to Covid-19 what second engines are to a 777. You probably don’t need a mask 99.99% of the time, but it’s sure great to have one on when you need it.
Another important thing we know now about Covid-19 is that outbreak severity is different from region to region. In a long and ultimately satisfying New Yorker article, Siddhartha Mukherjee explores how much we know and how little we understand about difference in Covid-19 outbreaks. As Mukherjee explains, scientists try to model Covid-19 cases and deaths based on a myriad of factors like demographics, population density, public health systems, and climate. None of the models predicts India and Pakistan accurately. None of them get Nigeria right. So, what is it that makes Covid-19 super deadly around Milan and London while it’s more like a mild flu in Lagos or New Dehli?
It could be environment (e.g., warmer places have more ventilation). Perhaps public health systems and overall fitness of a population explain the differences. Many places misreport Covid-19 by as much as 20% – 30%, so maybe reporting skews differences. Is it age demographics? India has a much lower mean age than Italy. Scientists have started considering whether Covid-19 shares traits with earlier viruses that produce a cross-reactive immune response. Many of these factors have at least some correlation to Covid-19 infections and deaths, but none is the silver bullet the explains the range of viral responses in different places.
The fact is that Covid-19 is a vastly different disease in different communities. That makes it hard to compare, say, the effect of different Covid-19 policies on different local economies because different regions have such different Covid-19 outcomes even when they have similar policies.
As researchers improve their models, parsing all these factors in India, Pakistan, Nigeria, and elsewhere, we will learn things about transmission that contradict public health advice during the pandemic. Already, one study already says that businesses didn’t need to close if they’d followed masking, distancing, and ventilation guidelines. In India, even those restrictions don’t appear to be necessary. Businesses there haven’t closed and, practically speaking, there are no Covid-19 restrictions, yet India’s Covid-19 mortality is low.
I suspect there will be many I-told-you-so’s as transmission is better understood. After all, when all is said and done, California and Florida have arrived at about the same place in terms of Covid-19 cases and deaths even though they adopted significantly different restrictions. It’s too early to say that policy didn’t matter and it’s important to remember the lives lost from throwing public health guidelines out the window for the sake of the economy. The meat packing industry is a good example of an industry that flaunted guidelines, lost many of its employees to Covid-19, and spawned outbreaks in communities around its meatpacking plants.
All this brings me to my main point: Covid-19 misinformation. I’m going to start the Covid-19 misinformation portion of today’s post with a quick story about a diversity training seminar I attended. In one of the exercises, the instructor wrote a sentence on the whiteboard and asked each of us to write down on a piece of paper how many times the letter “e” occurred in the sentence. That seemed stupid, but everyone wrote down the number of times “e” occurred in this sentence.
Then the instructor asked how many participants wrote down “1.” No hands. She asked who wrote down “2.” No hands. Then “3.” A few hands went up. The “4.” Some other hands went up. And so on.
The point was that participants looking at the same sentence saw it in different ways. The subjective experience of the sentence was different from the objective sentence. That’s important in understanding diversity, of course, but also for understanding a key aspect of misinformation. If we were to get invested in our first perception, which we are likely to do, we may end up with a cognitive bias. Even when provided evidence that an initial perception is incorrect, people may continue to advocate it if only to save face.
Social media compounds our initial (mis)perception by reinforcing it with messages we want to hear. Once you have taken a stance and are saving face, sharing stories that support your stance lend credence to your cause. In this way, the propagation of misinformation on social media may be a larger long-term public health problem than Covid-19.
Short-term, it’s likely that social media is keeping some people locked into their Covid-19 vaccine misperceptions. As our understanding of Covid-19 transmission has evolved and as public health policies have changed, it’s easy to assert that no one really knows anything. But public health is changing in response to more and better Covid-19 information (e.g., airborne transmission and superspreader events).
It’s more significant when the people thriving on misinformation are healthcare providers who influence medical decisions. Mother Jones investigated nurses’ social media groups and found rampant sharing of vaccination misinformation.
It’s not hard to find vaccination misinformation online. Even when Youtube and other platforms remove misinformation videos, misinformation purveyors make their videos available on their own websites and leverage social media to drive traffic to those sites. The sales pitch during these videos is akin to an MLM get-rich-quick scheme.
Anti-vaxx is big business. The Centre for Countering Digital Hate estimates that social media companies rake in about US$1 billion in ad revenue for anti-vaxx ads. Two groups fund over half the anti-vaxxer ads on Facebook, the World Mercury Project, chaired by Robert F Kennedy Jr., and Stop Mandatory Vaccinations, owned by Larry Cook.
Who is Larry Cook? He’s a former sound technician and was Executive Director of the California Naturopathic Doctors Association from 2012 to 2016. He is now what I would call a social media influencer, someone who makes his money promoting healthy lifestyles on social media platforms.
Having worked in the social media influencer business, my guess is that Cook raises money for anti-vaxx ads, takes a cut of the donations, and drives traffic to places where he not only provides anti-vaxx misinformation, but also sells merchandise. What separates Cook from someone like Steve Bannon, who misappropriated donations for building a border wall, is that Cook doesn’t promise to deliver anything. Cook’s business model probably looks like the NRA, whose executive staff waves the American flag while it lines its pockets with donations derived from fear mongering gun rights misinformation.
The business model problem is that social media companies don’t want to lose US$1 billion in revenue. I am one of the people who don’t see anti-vaxx ads because they’re targeted for anti-vaxxers, but Cook and others create a self-reinforcing echo chamber of anti-vaxx information. Social media algorithms thrive on targeting anti-vaxx content. The communities they create online have real world consequences.
While social media platforms earn US$ billions and a few influencers make bank on Covid-19 misinformation, the social costs are devastating. The Director of the NIH, for instance, says he can make a case the tens of thousands of lives were lost to Covid-19 because of the politicization of masks.
One last word about Covid-19 misinformation: privilege. Last week I wrote about how Covid-19 reveals who we are. Those who advocate against Covid-19 vaccines in the face of overwhelming evidence how much disease and suffering they prevent are usually in a position of privilege. Not privilege in the sense of having money, but privilege in the sense of not wearing a motorcycle helmet or seat belt. It’s the privilege of saying, in effect, if my misinformed decision fails me, I expect those who listened to and followed expert advice to take responsibility for my decision.
Covid-19 bits.
- Prime Minister Boris Johnson announced a four-step program to end Covid-19 restrictions starting 12 April.
- Spanish hotels are seeing a spike in summer bookings. Most of Spain’s tourists are from the UK.
- The last remaining male member of the Juma tribe on the Amazon River died from Covid-19. He is survived by three daughters.
- A Texas judge struck down a Covid-19 eviction moratorium, putting more minority communities at higher risk during the pandemic.
- About 1/3rd of US active military forces are declining a Covid-19 vaccination. This is creating national security risks during Middle East deployments.
- Last week, the CDC announced that Covid-19 reduced US life expectancy by a year. That calculation was incorrect. The pandemic has reduced US life expectancy by about a week.
- Hair loss is a symptom of Covid-19, even from the stress of worrying about infection.
- Scientists are proposing an antiviral approach to Covid-19 and other Coronaviruses that interferes with their reproduction proofreading mechanism, rendering them harmless.
- It appears that T-cells will protect against Covid-19 variants even if new variants navigate around antibodies developed from infection or vaccination.
- If booster shots for Covid-19 variants are needed, the FDA plans to treat them like flu vaccines, allowing smaller trials for approval.
- The US FDA approved an Emergency Use Authorization for the Johnson & Johnson Covid-19 vaccine. After 28 days, the single dose vaccine is 85% effective against severe cases and 100% effective against hospitalization and death.
I write Covid Diary BCN for my own sanity. If it helps you, please forward a link to friends and family. For more frequent Covid-19 updates, follow me on Twitter.

One thought on “28 February 2021 – Sunday – #136”
Comments are closed.