I was more than a little surprised to get this message from Bicing yesterday (translated from Catalan by Google Translate).
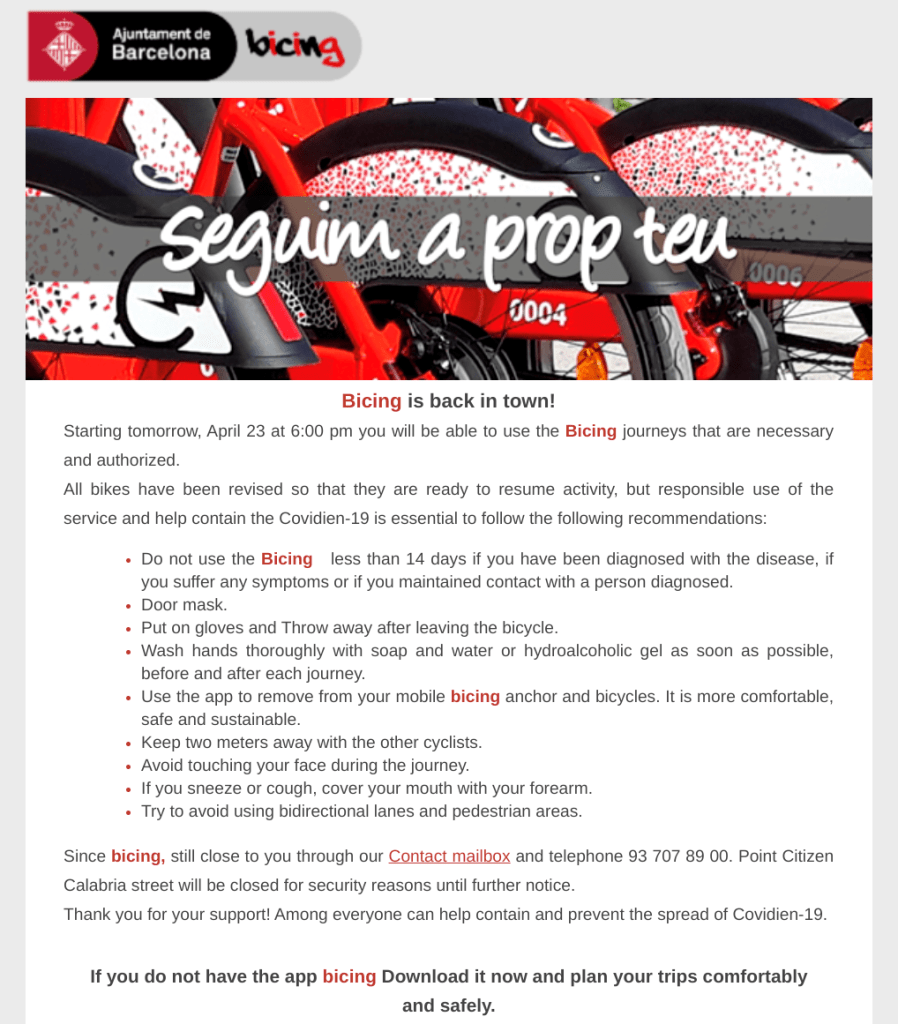
I wrote in a previous entry that one of my favorite things about Barcelona is Bicing, the bicycle sharing service. After a few years riding Citibike in New York City, seeing the Bicing bike stands when I visited Barcelona last summer made my decision to move here easy. I was sad to see Bicing mothball its service last month due to Covid-19.
Now that Bicing is up and running again, I just need somewhere to bike to. Still waiting for Spain to let us out of our cages for at least a bit of exercise.
Two statistics I want to discuss today. One is the Covid-19 mortality rate, the other is the Covid-19 Infection Fatality Rate (IFR).
By now, if you haven’t seen any of the Financial Times Covid-19 charts, you’ve been sleeping much more than I have. The guy behind all these dazzling charts is John Burn-Murdoch, who’d I assumed was a curmudgeon I’d run into in the bowels of the British Museum churning through spreadsheets, but turns out to be a rather telegenic bloke. Near the end of this useful Twitter thread about Covid-19 charts, Burn-Murdoch, which is such an ironic name for someone competing against News Corp, inserted this video explainer about decisions FT makes in presenting Covid-19 case and mortality data.
It’s hard to get accurate Covid-19 data that are consistent across regions and it’s hard to present them. Burn-Murdoch describes some of the issues he faces with Covid-19 data. For instance, making a distinction between Covid-19 cases and confirmed Covid-19 cases, and understanding that some governments are better than others at testing. One important takeaway from his Q&A is that Covid-19 data trends are predictive. That is, while the data may not be accurate, all countries’ Covid-19 outcomes resemble each other. The curves are converging.
One emerging story this week that demonstrates a problem with mortality data accuracy is the underreporting of Covid-19 deaths, mostly in jurisdictions whose healthcare systems have been overwhelmed by Covid-19. My cousin Nancy passed on the chart below, but New York Times and other sources have reported similar death reporting discrepancies.
Eyeballing the countries on this graphic, it looks like about 26k deaths were underreported worldwide. Covid-19 deaths worldwide are at about 176k right now, which puts the worldwide undercount around 13%.

I’d pull out my spreadsheet and calculate the exact percentage except that I want to make the point that most Covid-19 data don’t have eighteen places of accuracy. If you get within a percent of the right number these days, you’re doing well.
A mortality undercount means we may have underestimated Covid-19 morbidity. As good as our models may be, they’re only as good as the data. Over time models and data improve. It’s important to acknowledge we have a ways to go.
On the IFR front, my social media streams are hot with assertions that Covid-19 IFR is about the same as seasonal flu because of recent studies of Covid-19 infection rates in Santa Clara County and Southern California. These assertions are usually in the context of, see, we really don’t need lockdowns.
Here’s a good Twitter thread that covers IFR data from UK, China, South Korea, and the Diamond Princess cruise as well as a new study from Geneva.
While Gardiner estimates a Covid-19 IFR of 1.1% with a confidenc interval of 0.5% to 2.5%, the Centre for Evidence Based Medicine comes in with a lower Covid-19 IFR confidence interval of 0.1% to 0.36%, a confidence interval whose highest estimate (0.36%) is lower than Gardiner’s lowest estimate (0.5%). Unlike Gardiner, the CEBM numbers exclude Geneva, but include Iceland. I suspect that the different regions under consideration have less impact on the two different Covid-19 IFR confidence interval estimates than the different estimate methodologies.
I write all this about IFR to point out that when I read social media posts that claim the real IFR is such-and-so based on the most recent measurement made wherever, I strongly suspect someone is trying to make a case along the lines of all lockdowns are bad (or good). I’m not about to trust my social media feeds when even the experts are having trouble converging on an IFR number. One reason for IFR uncertainty may be the undercount of deaths mentioned above. Another possibility that’s emerging (see yesterday’s entry) is that different strains of Covid-19 seem to have spectacularly different virility, meaning we may start seeing regional IFRs emerge based on the dominant Covid-19 strain.
One of the reasons I’m spending time on mortality and IFR today is I’m reading lots of assertions based on these data, often with a reference to some sketchy blog (not this one!) or a random quote. There are assertions that the cost of the Covid-19 lockdowns is higher (in death or money) than the cost of letting Covid-19 run its course. There are assertions that mortality rates are higher than we thought or lower than we thought. There are calls for all of us to use our critical thinking skills so we’ll agree with what someone has just posted!
In times of uncertainty, we all want answers. But before we even get to critical thinking, here’s a simple set of rules from University of Washington on how check something before you post.
- Stop when something moves you to post
- Investigate the source
- Find better coverage
- Trace Claims, Quotes, and Media to the Original Context
When I write about something, I try to find a trusted source and confirmation. I don’t always find those, but my agenda here is about getting things right. It’s what got me through the AIDS crisis. Often the search for sources and confirmation takes me down paths to different stories of interest, so part of where I’m exerting editorial control is by excluding what I think is irrelevant to an entry. I hope part of the value I add is developing a sense of the importance of a story at any given time in the enormous context of the Covid-19 pandemic.
For now, I’m taking claims based on Covid-19 mortality rates and IFR with a large grain of salt. What we know works is social distancing, hand washing, and testing. What we don’t know with enough precision to make decisions is Covid-19 mortality rate and IFR.
Sorry I got all high and mighty about sourcing. That allows me to sink innocently into some pure speculation about blood type, blood clots, ACE inhibitors, and testicles. Now that I’ve got your attention, these are all subjects I plan to write about in the next couple of days. I’m just going to say that (cover your eyes if you’re squeamish) it looks like men may have a higher mortality than women because their testicles are a reservoir for Covid-19 and so be careful having oral sex! Just speculation, mind you.
Books. I knew you wanted an update on books, so welcome to the book corner.
First off, I sent the final revision of Dear Mustafa to my editor yesterday. Yea!
Writing yesterday about how the earliest US Covid-19 cases probably were in Santa Clara County rather than Kirkland, Washington, I was reminded of Randy Shilts’ Patient Zero conceit in his book And the Band Played On: Politics, People, and the AIDS Epidemic. Shilts annoints Canadian flight attendant Gaëtan Dugas as Patient Zero and follows his sexual exploits as way of educating readers about the early spread of HIV. For the record, I had dinner with Randy at some random AIDS benefit in San Francisco.
Before Covid-19, small bookstores were making a comeback. In this interview, Peter Mulvihill from Green Apple Books talks both about his struggle to keep his three San Francisco stores open during the Covid-19 pandemic and about what people are reading. [Hint: think plague]. It’s a great view into the day-to-day problems of trying to keep a small business afloat.
Finally, Happy Sant Jordi Day from Barcelona! My friend Laura reminded me that, along with everyone else, I’m missing Barcelona’s Sant Jordi book festival because we can’t have one this year. Barcelona has book stores everywhere, which, in addition to Bicing, is another reason I was attracted to the city. This also was the first year New York City was going to adopt the Barcelona tradition, so I guess I could have celebrated Sant Jordi there if I hadn’t moved to Barcelona. Alas, I have my Bicing bike again but no bookstores to visit.