A lot of the chatter in my social media feeds is about whether the US has turned the corner and whether the lockdown is worth its economic consequences.
It’s worth noting that Covid-19 mortality charts comparing countries mostly have changed their data presentation from units of deaths to units of deaths per capita.
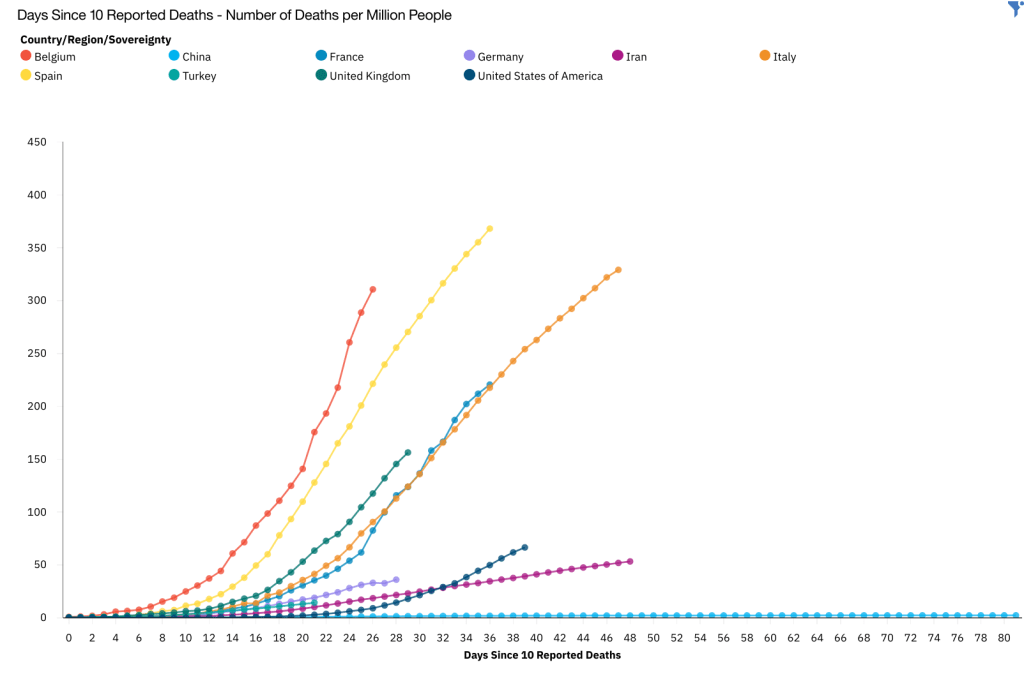
The switch in vertical axis units was needed, of course, because US deaths were swamping deaths in other countries.
On 31 March, I estimated 350,000 – 500,000 US Covid-19 fatalities based on an assumption that the US per capita Covid-19 death rate would be similar to another estimate I made for Italian per capita deaths. At that point, I was watching New York and assuming the rest of the US would follow suit. Obviously in states like California that locked down earlier, the US has not followed suit.
Two weeks later, I can see what I hope is an inflection in the US mortality curve. I still think the US is susceptible to new hot spots in a way that countries with complete lockdowns are not, and so I think any inflection in the US curve is at risk.
Parenthetically, I wonder if the US car culture has anything to do with its Covid-19 performance versus European countries. It may simply be that most of the US didn’t max out its healthcare infrastructure, but it seems like there may be other factors at play.
I compared US Covid-19 mortality per capita to a different set of countries here.
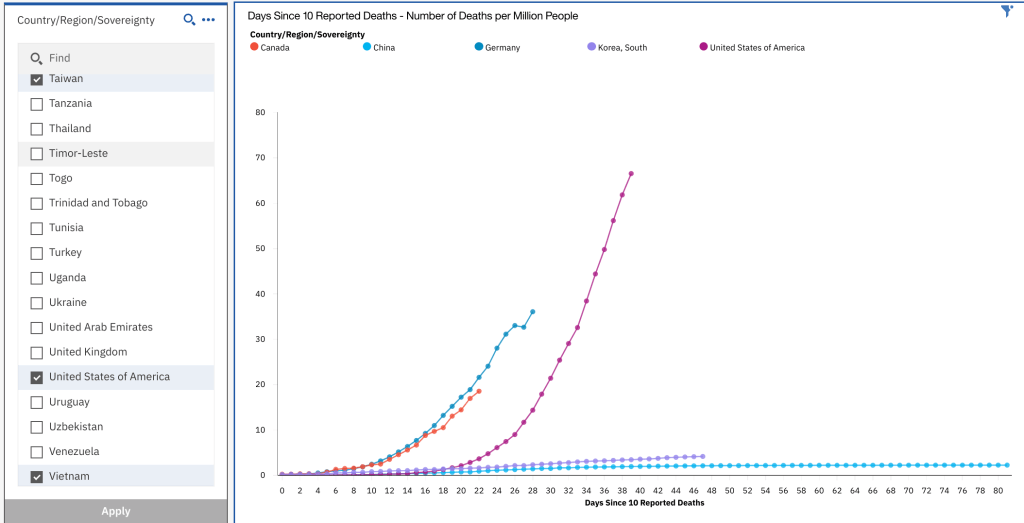
This chart shows how the US performed against countries that had the most effective Covid-19 responses. I show on the left that I included Taiwan and Vietnam. Those two countries’ Covid-19 responses were so good, they don’t register on the chart.
Clearly, South Korea and China had much better responses than the US, although there are disputes about the accuracy of Chinese mortality data. Germany and Canada may be the closest cultural comparisons in terms of governing style, although neither is as large and diverse as the US.
I think it’s fair to say that the US, which had earlier notice and better resources than most countries, responded poorly. As of today it has 2x – 10x higher per capita Covid-19 mortality than the best responders. There is more upside risk in that multiplier than downside risk.
In the same way that scientists are working on Covid-19 treatments and vaccines at a blinding pace, economists and policy wonks are churning out economic recovery plans. The push to open up the economy is a difficult trade-off over many variables. The phrase “open up the economy” sounds to me like we closed a door in March and, if we just open that door, the world will be what we remember from six months ago. There is no such door and the world will not be the same.
Brad tipped me off on what I would consider an optimistic timeline from Morgan Stanley.
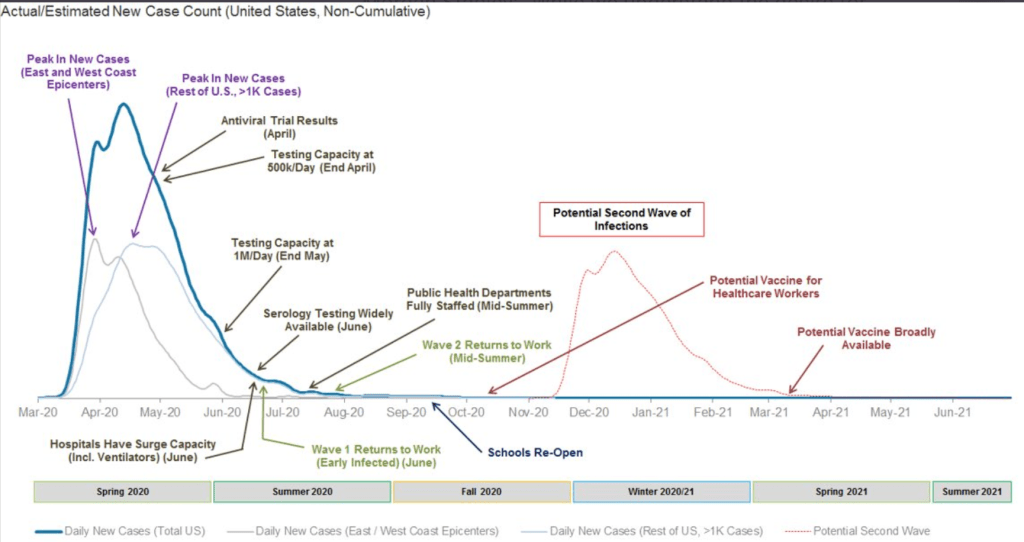
The Morgan Stanley timeline assume working vaccines in the US within a year.
“While we understand the desire for optimism, we also caution that the US outbreak is far from over. Recovering from this acute period in the outbreak is just the beginning and not the end. We believe the path to re-opening the economy is going to be long.”
Morgan Stanley Covid-19 recovery report
Most recovery plans imagine a very different world, a world with mass testing or mass tracking, or both. Any plans require cohesive international leadership to scale globally. The US might have been able to lead such an effort four years ago, but its leadership can’t even get American citizens on the same page about something as straight forward as social distancing. Even if international leadership rallies behind a cohesive plan, it still faces a far-right challenge in the US and elsewhere to leverage Covid-19 to tear down existing government structure.
Minorities and the poor will suffer the worst consequences of opening up too soon. There are arguments that the economic harm from worldwide lockdowns will kill more minorities and poor people than Covid-19 itself. Most of the people I know making this argument make it from a position of privilege. I not sure the trade offs are being made fairly in any argument to open up the economy right away.
It is clear that minorities and the poor are already getting the short end of the Coivd-19 stick during the lockdowns. Low wage earners with essential jobs usually face more Covid-19 risk because they don’t have the luxury of working remotely at home. Jails and immigration holding facilities have failed to provide adequate healthcare to their laregely minority and poor populations. The US healthcare system, which normally doesn’t work well for minorities and poor, is failing minorities during the US Covid-19 outbreak.
The parts of the supply chain that are working are not safe for low-wage workers who staff them. Opening up the economy will put disproportionately more low-wage workers at risk of Covid-19 infection. Opening up the economy also will test crippled international supply chains which operate in underdeveloped countries that are further behind in their Covid-19 epidemics.
I wish I could wave a wand and say open up the economy today. European and US Covid-19 are looking good. Everyone wants to step outside. How bad could it be if everyone starts working again?
In my opinion hydroxychloroquine offers an object lesson in how easy it is to promote a simple solution that turns out not only to be wrong, but hurts people.
For those of you keeping tabs, there are no hydroxychloroquine breakthroughs. Dr. Didier Raoult, the French doctor who first claimed miracle results and, as far as I can tell, is the epicenter of the hydroxychloroquine drama, now claims to have a 98% cure rate in over a thousand patients with no cardiac toxicity. The claim is made without a published study or a control group. This is similar to the other quack doctor advocating hydroxychloroquine, Dr. Vladimir Zelenko in New York, who claims hundreds of successful outcomes. Dr. Zelenko also hasn’t presented a full study and has no control group.
In what appear to be leaked results of a study from Detroit, hydroxychloroquine does not benefit Covid-19 patients. With 63 patients, the study is too small to draw conclusions. However, the patients were divided into half that got hydroxychloroquine and half that did not, so this study has a control.
A Brazilian study halted high dose chloroquine testing because of cardiac toxicity. The study is continuing with low dose chloroquine testing. The Brazilian study has 81 patients and includes azithromycin and ceftriaxone antibiotics. So far, the mortality results for patients on chloroquine is about the same as general Covid-19 mortality, so it doesn’t appear to have a benefit.
Finally, in a non-Covid study looking at case data across six countries for complications in rheumatoid arthritis patients from use of hydroxychloroquine with different antibiotics, use of hydroxychloroquine with azithromycin appears to increase risk of angina and heart failure by 15%-20%. Azithromycin is the antibiotic recommended for use with hydroxychloroquiine in Covid-19 patients.
The bottom line is that there are many Covid-19 treatment candidates and there is nothing concrete so far to suggest that hydroxychloroquine is a standout among them. In fact, it appears that hydroxychloroquine poses significant cardiac risk when used with azithromycin and possible cardiac risks otherwise if dosage is not managed correctly.
I suspect that if hydroxychloroquine were a magic bullet, we would have more anecdotal evidence that’s true and at least hints about a well done study with promising results. We have a lot of usage, but we have neither overwhelming anecdotal reports nor whispers of a good study.
But we didn’t hurt anything by trying hydroxychloroquine, did we? The president’s message that hydroxychloroquiine is the magic bullet for Covid-19 has disrupted supplies for people who already use it for malaria and lupus. Guess who that hurt. Minorities and the poor.
